Share on Facebook
Share on Facebook Share on X
Share on X Share by Email
Share by Email Share on Google Classroom
Share on Google Classroom
From the 17th century until about 1900, hospitals in what is now Canada were unspecialized, multi-purpose institutions for the sick poor. Until around 1900 those able to pay doctors preferred to be treated at home. The first hospitals emerged in places where people were unable to get medical treatment by physicians in their own homes.
The financial sources and social mandates of hospitals have varied widely over the past 400 years. The earliest hospitals included military and marine hospitals, as well as Roman Catholic and then Protestant benevolent institutions. By the turn of the 20th century, the administration of scientific medicine was the major purpose of the Canadian hospital. Since about 1970, hospitals have become increasingly specialized; structurally they have become flexible and expandable.

New France
In New France, urban institutions intended for healing were first housed in temporary wooden buildings. The Hôtel-Dieu in Montréal, for example, was a small building (24 x 60 feet) established in the fort at Ville-Marie in 1644 (see Hôtel-Dieu). According to the first annalist, Soeur Morin, it contained two sick wards, a kitchen, rooms for servants and for founder Jeanne Mance.
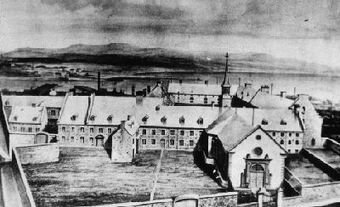
The first hospitals were sites where the proselytization of Indigenous peoples by religious nursing sisters was carried on. Later, colonists were accepted as patients and offered more permanent quarters in generic (i.e., unspecialized) masonry buildings. The Hôtel-Dieu in Quebec City, established in 1639 by Augustine nursing sisters, was given its first permanent stone building in 1658. This single-storey, gable-roofed structure contained one ward of 10 beds connected to a chapel, allowing the patients to hear mass. In 1672, a second, 24-bed ward was added and patients were segregated by gender. Hospitals such as this were connected to convents; windows in the 1672 Hôtel-Dieu looked directly onto the convent courtyard. Technologically advanced for its time, the Hôtel-Dieu had running water in the wards and latrines through a system of lead and stone ducts. Following a series of fires in 1725 and 1755, the Hôtel-Dieu was rebuilt in 1816-25. Other early hospitals established at Trois-Rivières (1697), Hôpital Général de Québec (1692) and Hôpital Général de Montréal (1694) took care of the aged poor and orphans, in addition to the sick.
The pattern of replacing rudimentary quarters with more solid buildings was followed throughout New France. Louisbourg, Cape Breton, originally included a crude hospital on the north shore of the harbour. In 1730, the Hôpital du Roi was completed, featuring its own chapel, morgue, apothecary, bakery, laundry, kitchen, latrines, and wards for members of the Brothers of Charity, the medical order which ran the institution. An anonymous soldier described the Louisbourg hospital in 1745 as a two-storey masonry structure and yard, surrounded by a massive wall, 12 feet high and 4 feet thick.
Atlantic Coast
The Atlantic coast was also the site of special hospitals for sick mariners, who did not have the option of home care. Marine hospitals were mostly constructed in the early 19th century and closed in the late 19th and early 20th centuries, as other institutions began to accept non-residents as patients. Six such institutions were built before Confederation, five in New Brunswick and one in Quebec City. The Marine Hospital in Douglastown, New Brunswick, a single-storey, rectangular sandstone building, is a good example of this type of hospital. It had a low-pitched, hipped, slate roof, crowned by a domed cupola. The scale of the hospital's operations was relatively small. During its early years, the Marine Hospital in Douglastown accommodated 10-12 seamen who were treated by three physicians.
Early Urban Hospitals
The 19th century also saw the construction of much larger lay general hospitals in Canada's growing cities, such as the Montréal General Hospital (MGH, 1821), the Toronto General Hospital (1824), the Victoria General in Halifax (1859) and the Vancouver General (1886). These Protestant, benevolent institutions were often sited at some distance from the city centre (although the cities soon engulfed them), for the protection of both the patients and the healthy population.
Many of these early 19th-century hospitals-the original MGH, the Kingston General Hospital (1835) and Toronto (York) General Hospitals-resembled large country houses. They were rectangular structures with central entries. The MGH, designed by architect Thomas Phillips, was a three-storey building crowned by a classical cupola which illuminated its first operating room. All three hospital roofs were hipped and punctuated by numerous chimneys.
Throughout the 19th century, larger hospitals were constructed and existing hospitals were extended. The MGH was enlarged with the Richardson and Reid wings in 1832 and 1848, respectively. Some new institutions, such as Montréal's Royal Victoria Hospital (1894), designed by H. Saxon Snell, showed the direct influence of British hospital planning. Its central administration block was framed by long, narrow wings for medicine and surgery. These featured open wards shared by 32 patients, known as Nightingale wards, which culminated in generous sun porches and sanitary towers.
Such hospitals accommodated student nurses, pathology departments, surgical amphitheatres, small wards and private rooms. Whereas nurses had lived in rooms scattered throughout the hospital proper for most of the 19th century, early 20th-century hospitals saw the construction of purpose-built nurses' residences. During the 1920s these residences began to include teaching facilities in addition to individual rooms. Nurses' residences, designed to attract middle-class women to the profession, often resembled large houses. Their prominent silhouette in hospitals such as the Royal Victoria and Notre-Dame hospitals in Montreal, Kingston General Hospital and Ottawa Civic Hospital express the institution's recognition of the important role nurses played in the hospital.

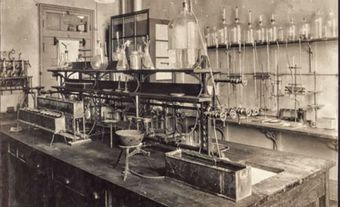
Both pathology departments and surgical amphitheatres in 19th-century hospitals doubled as teaching facilities. The Fenwick Operating Room in the Kingston General Hospital opened in 1895 and was considered one of the "finest equipped operating rooms of its kind in America." It was typical of the growing orientation of the Canadian hospital towards surgery. Designed by architect William Newlands, the semicircular Fenwick Operating Room was white, with walls of polished marble and a slate floor, reflecting the widely held belief following the development of the germ theory that easy-to-clean materials were aseptic. This misconception was accompanied by a mania for natural light and a continuing demand for fresh air. At the Fenwick Operating Room, natural light poured through large skylights and was then diffused through a ceiling of ground glass.
Early 20th-Century Hospitals
Early 20th-century hospitals, in comparison with their predecessors, were massive and compact buildings featuring smaller wards and specialized spaces arranged along double-loaded corridors. By this time the increasingly specialized profession of medicine demanded custom-designed facilities for laboratories, X-ray and other diagnostic functions, as well as physio-therapy, hydro-therapy and electrotherapy. Support services for medicine also appeared at this time in hospital plans, especially for record-keeping and laundry. Suites of smaller rooms designed for surgery, often separated from patients' rooms, replaced the now outdated surgical amphitheatre.
Rather than reflect the stark, undecorated tenets of International Modernism, Canadian hospitals before the Second World War typically mirrored their local or regional architectural traditions, perhaps an indication of the conservatism of their administrators and patrons. The architects who modernized Kingston General Hospital in 1916-31, for example, deliberately modelled their design on the historic main building. It had accommodated the first meeting of the United Legislature of Canada during 1841-44.
Another example of this triumph of regional traditions over International Modernism is the expansion of Montréal's second Hôtel-Dieu by architects Dalb, Viau and Alphonse Venne in 1925-33. They added a fireproof wing with 60 beds which purposefully recalled the classical, domed monument designed by Victor Bourgeau in 1859-61.
Early 20th-century hospitals also satisfied the needs of new users: paying patients. Private hospitals, for example, boasted more luxurious materials and included smaller wards and single rooms, entries designed for the automobile, and elegant lobbies. Toronto General Hospital's New Private Patients' Pavilion of 1930, designed by Darling & Pearson, was a 9-storey tower, T-shaped in plan. It included interiors panelled in fine woods, Persian carpets and radio headphones at every bed, among other costly features.
Whereas women and children had been cared for within the 19th-century hospital, a virtual boom of specialized buildings intended for their needs followed the First World War. Prewar structures, such as Montreal's Children's Memorial Hospital (1909), were romantically situated in "natural" settings and focused mostly on orthopedics. Obstetrics was the specialty designed around women's health needs. Toronto's Women's College Hospital (1911, 1915, 1935) marked the growing awareness of women's special health needs and was a significant site for the education of women physicians in Canada.
Hospitals after the First World War
The period following the First World War was the golden age of the Canadian hospital. By this time, the design of hospitals was highly specialized within the profession of architecture. The firm of Edward F. Stevens and Frederick C. Lee, for example, with offices in Boston and Toronto, designed more than 25 per cent of the country's accredited institutions. Other notable Canadian architects of hospitals during this period were B. Evan Parry, James Govan and J.C. McDougall.
While the overall design of new hospitals was frequently the responsibility of these internationally known experts, hospital construction was almost always overseen by a local architect. And these expert consultants were sometimes physicians, rather than architects. S.S. Goldwater of New York, for example, consulted on the Jewish General Hospital of Montreal, the Vancouver General Hospital, the Toronto Western Hospital and the Hamilton General Hospital.
Many Canadian hospitals lagged behind these ideals and made do with ad hoc quarters. During epidemics and wartime, for example, houses, factories, prisons, convents and even tents accommodated sick Canadians. During the 1920s and 1930s, Red Cross outpost hospitals occupied houses and train cars. And most hospitals began in quarters intended for other uses. St Joseph's Hospital of London, Ontario, for example, typical of institutions founded before Second World War, was originally housed in a residence with 10 beds.
Hospitals After the Second World War
After the Second World War, Canadian hospital construction exploded. Whereas in 1945 there had been 536 public general hospitals in Canada, 15 years later there were 844. The number of beds increased by nearly 88 per cent during this time period. Hospitals built in the 1950s were freestanding, high-rise towers, often surrounded by parking facilities. One example of this type of hospital is the Calgary General Hospital by W.L. Somerville, McMurrich and Oxley. The hallmarks of the hospitals after the Second World War were standardized floor plans, undecorated façades, flat roofs, vertical circulation and controlled ventilation. Their massing often comprised clear rectangular volumes colliding at right angles. The image of Canadian hospital after the Second World War was sleek and modern, whereas the interwar institution had been romantic and highly decorative.
Hospitals since about 1970 have reached an unprecedented size and their building programs are increasingly sophisticated. A primary concern of architects has been the need to design for anticipated changes of function. The introduction of the "interstitial service floor," which permits aspects of the building infrastructure, previously immoveable, to be rearranged quickly, has been an important design response to this new requirement. Interstitial service floors were first introduced at the Mcmaster Health Sciences Centre in 1972 and further developed at the Mackenzie Health Sciences Centre in Edmonton in 1986.
Recent Trends
So-called "superhospitals" are in the planning stages in a number of Canadian cities. These enormous megaprojects call for the abandonment of historic hospital buildings and the re-accommodation of several institutions in a single structure in order to prevent the duplication of services. The Halifax Infirmary building (1997) of the QEII Health Sciences Centre in Halifax and the proposed McGill University Health Centre in Montreal are examples of this trend.

Many new Canadian hospitals are also designed for "patient-focused care" - the bringing of medical services directly to patients in private, multi-purpose, homelike rooms, rather than transporting them to specialized units throughout the institution. Toronto's Hospital for Sick Children was designed in 1993 by the Zeidler Roberts Partnership to deliver this kind of care (see Eberhard Zeidler). The designs of these buildings often resemble shopping malls or office towers, with individual departments facing onto generous circulation spaces or even atriums.
The design requirements for Canadian hospitals have come full circle. While the first European settlers to Canada preferred to be treated by physicians at home, drastic cuts to healthcare budgets across the country have resulted in a rise in "homecare."Shorter hospital stays and greater reliance on outpatient clinics have meant that many hospitals offer only acute care while others have been renovated for other uses, or abandoned.
See also Hospital.